As full-thickness wounds heal, they begin to fill in from the bottom upward with granulation tissue. At the same time, wound edges contract and pull together, with movement of epithelial tissue toward the center of the wound (contraction). These epithelial cells, arising from either the wound margins or residual dermal epithelial appendages within the wound bed, begin to migrate in leapfrog or train fashion across the wound bed. Horizontal movement stops when cells meet (contact inhibition). The ideal wound edge is attached to and flush with the wound bed, moist and open with the epithelial rim thin, and pale pink to translucent.
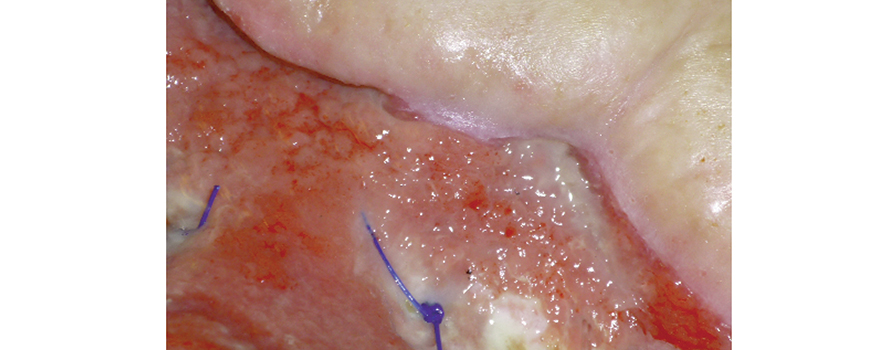
In many chronic wounds, a problem with slow or absent epithelial edge advancement is caused by a clinical condition known as epibole. Epibole refers to rolled or curled-under closed wound edges that may be dry, callused, or hyperkeratotic. Epibole tends to be lighter in color than surrounding tissue, have a raised and rounded appearance, and may feel hard, rigid, and indurated.
Causes
Epibole results when the upper epidermal cells roll down over the lower epidermal cells and migrate down the sides of the wound instead of across. Edges that roll over ultimately cease migration secondary to contact inhibition once epithelial cells of the leading edge come in contact with other epithelial cells. In other words, the body thinks the wound is healed and epithelial migration across the top of the wound ceases. There are many possible reasons why the epidermal margin fails to migrate, including hypoxia, infection, desiccation, dressing trauma, overpacking the wound bed, unhealthy wound bed, inability to produce the basement membrane that the epithelial cells adhere to, or cellular senescence.
Prevention
Follow these tips to help prevent epibole:
• Pack dead or empty space in the wound bed. Packing promotes healing from the bottom up and avoids abscess formation at the wound depth. Fill the depth of the wound to the surface. Do not pack tightly, as this will cause pressure and impair circulation. Wound fillers, hydrogel impregnated gauze, alginates, or fluffed plain-woven moistened gauze can be placed loosely into the space.
• Protect periwound skin with a skin sealant, moisture barrier ointment, or barrier wafer.
• Prevent epidermal stripping by using silicone border dressings or silicone tape; consider tape-free securement strategies.
• Protect the wound from pressure.
Treatment
Treatment for epibole involves reinjuring the edges and opening up the closed tissue, which renews the healing process. Options include conservative or surgical sharp debridement, treatment with silver nitrate, and mechanical debridement by scrubbing the wound edges with monofilament fiber dressings or gauze.
Nancy Morgan, cofounder of the Wound Care Education Institute, combines her expertise as a Certified Wound Care Nurse with an extensive background in wound care education and program development as a nurse entrepreneur.
Information in Apple Bites is courtesy of the Wound Care Education Institute (WCEI), © 2016.
Selected references
Black J, Baharestani M, Black S, et al. An overview of tissue types in pressure ulcers: a consensus panel recommendation. Ostomy Wound Manage. 2010; 56(4):28-44.
Ermer-Seltun J, Rolstad BS. General principles of topical therapy. In Doughty D, McNichol L, eds. WOCN® Core Curriculum: Wound Management. Philadelphia, PA: Wolters Kluwer; 2016; 107-30.
European Wound Management Association (EWMA). Position Document: Wound Bed Preparation in Practice. 2004; London: MEP Ltd.
Hamm RL. Evaluation of the patient with a wound. In Hamm RL, ed. Text and Atlas of Wound Diagnosis and Treatment. New York, NY: McGraw Hill; 2015;3:67-95.





